The Problem
Cranial Cruciate Ligament (CCL) injury is the most common injury causing clinical dysfunction in the dog. It is estimated that in 2003 pet owners in the United States spent over $1 billion for the treatment of damaged CCLs [1]. Surgical intervention is the treatment of choice primarily because of the inherent instability associated with the injury as well as the CCL’s inability to heal itself after being torn or damaged.
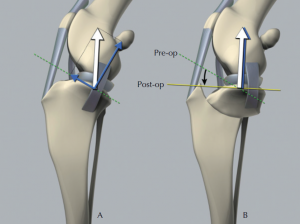
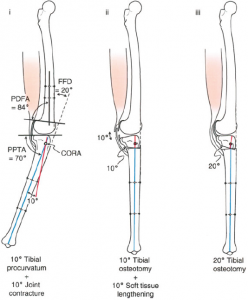
Numerous surgical procedures have been described for treatment of the CCL deficient knee in the dog. Most popular today are techniques that modify the mechanics of the dog knee by altering the anatomy of the proximal tibia such as tibial plateau leveling osteotomy (TPLO) seen in Figure 1. Dr. Don A. Hulse, D.V.M. at Texas A&M pioneered an alternate procedure that reduces the tibial plateau angle (TPA) by modifying the proximal tibial procurvatum using center of rotation of angulation (CORA) based leveling osteotomy (CBLO) which can be seen in Figure 2.
Testing
Numerous in vitro and in vivo studies have been conducted to evaluate instability of the canine knee following CCL transection. Instability generated with in vitro studies have shown 16-18 mm anterior translation and 8-10 mm proximal translation. However, instability generated through CCL transection with in vivo studies is approximately 10 mm anterior translation. The current in vitro model, seen in Figure 3, only accounts for forces that cause anterior translation of the tibia (gastrocnemius and quadriceps). The difference between the two models has lead us to believe the in vitro model to be inadequate, with respect to capturing the muscular complexity of the canine leg.
Improvements
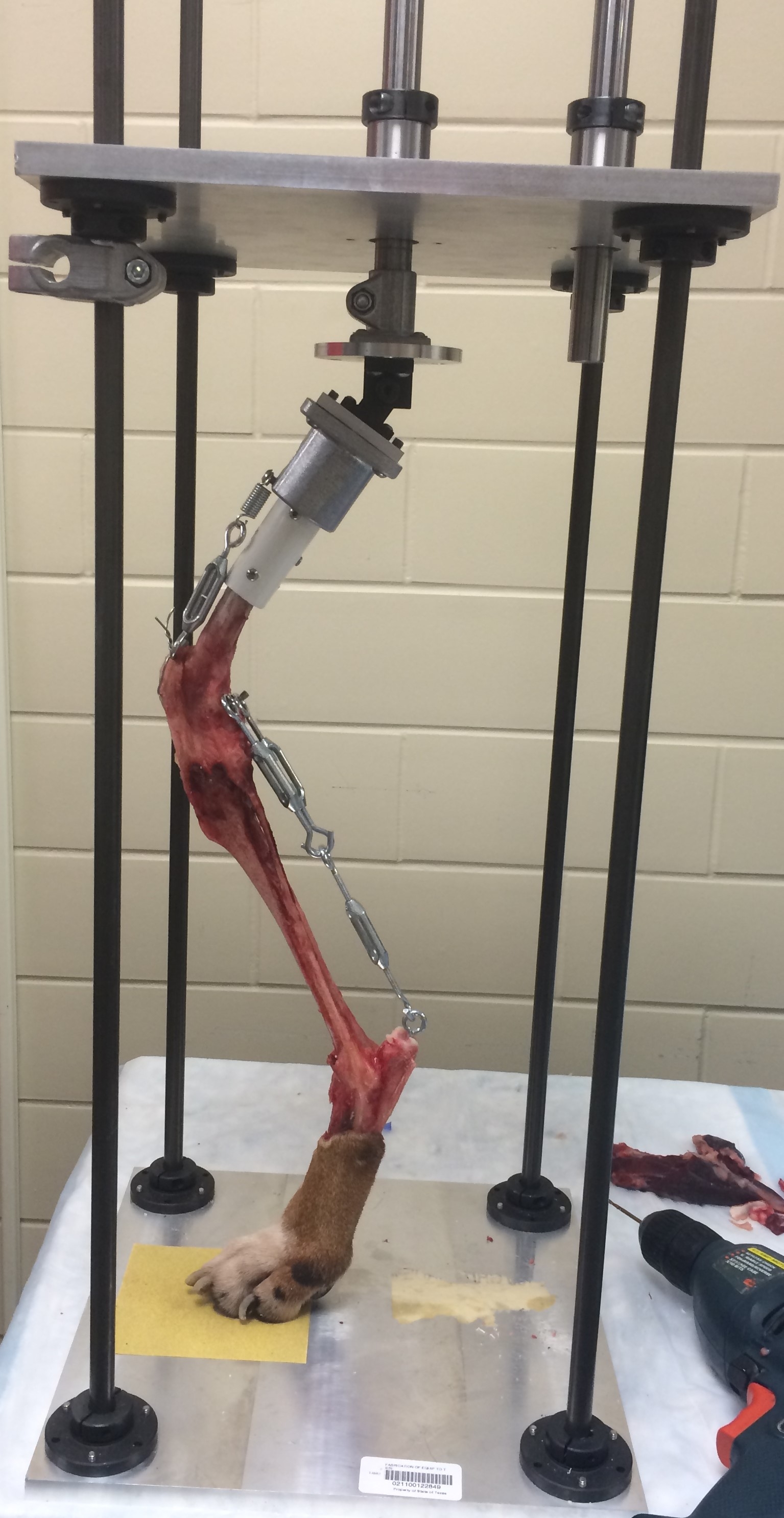
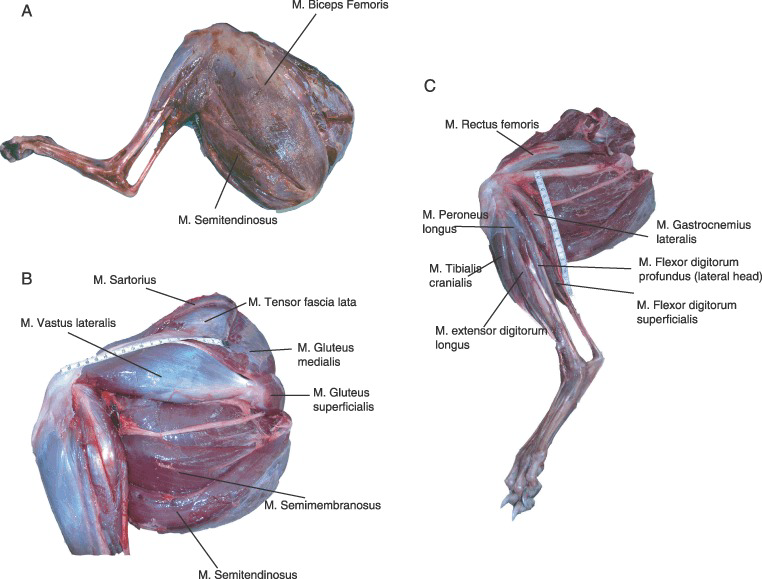
Researchers in the Biomechanical Environments Laboratory are working with lead surgeons in the department of Veterinary Small Animal Clinical Sciences (VSCS) to incorporate the muscles that prevent anterior translation of the tibia (Semimembranosus, Semitendinosus, Caudal Sartorius, Biceps Femoris) into the in vitro model which can be seen in Figure 4. Available literature will be used to identify the magnitude of the muscular forces related to low and normal levels of activity based on the canine weight. After properly identifying the magnitude of these forces, the muscular and skeletal anatomy will be analyzed to determine the origin and directionality of these forces. These biomechanical factors will then be modeled using various mechanical elements in the testing apparatus. The goal of this device is to better understand the instability of the canine knee joint after damage occurs to the CCL. By creating a biomechanically accurate in vitro experimental device, a better understanding of the resulting instability of the canine stifle joint can be acquired. This experimental device can then be implement further for controlled evaluation of surgical interventions used after CCL rupture for the determination of procedure efficacy.
References
[1] V. e. a. Wilke, “Estimate of the annual economic impact of treatment of cranial cruciate ligament injury in dogs in the United States,” J. of the Am. Vet. Med. Assoc., p. (Abstract), 2005.
[2] P. Muir, “Tibial Plateau Leveling Osteotomy,” in Advances in the Canine Craial Cruciate Ligaments, Ames, Iowa: Wiley-Blackwell, 2010, p. 170.
[3] P. Dror, “Sagittal Plane Knee Considerations,” in Principles of Deformity Correction, New York, Springer-Verlag Berlin Heidelberg, 2002, p. 524.
[4] S. Williams and A. Wilson, “Functional Anatomy and Muscle Moment Arms of the Pelvic Limb of an Elite Sprinting Athlete: The Racing Greyhound,” Journal of ANatomy, no. 213, pp. 361-372, 2008.